












A Picture of Health
In the award‑winning medical drama The Pitt, the work of treating America’s medical and social ills is allegorised in the television show’s unflinching confrontation with physical accidents, diseases and acts of God. Save to My Ocula

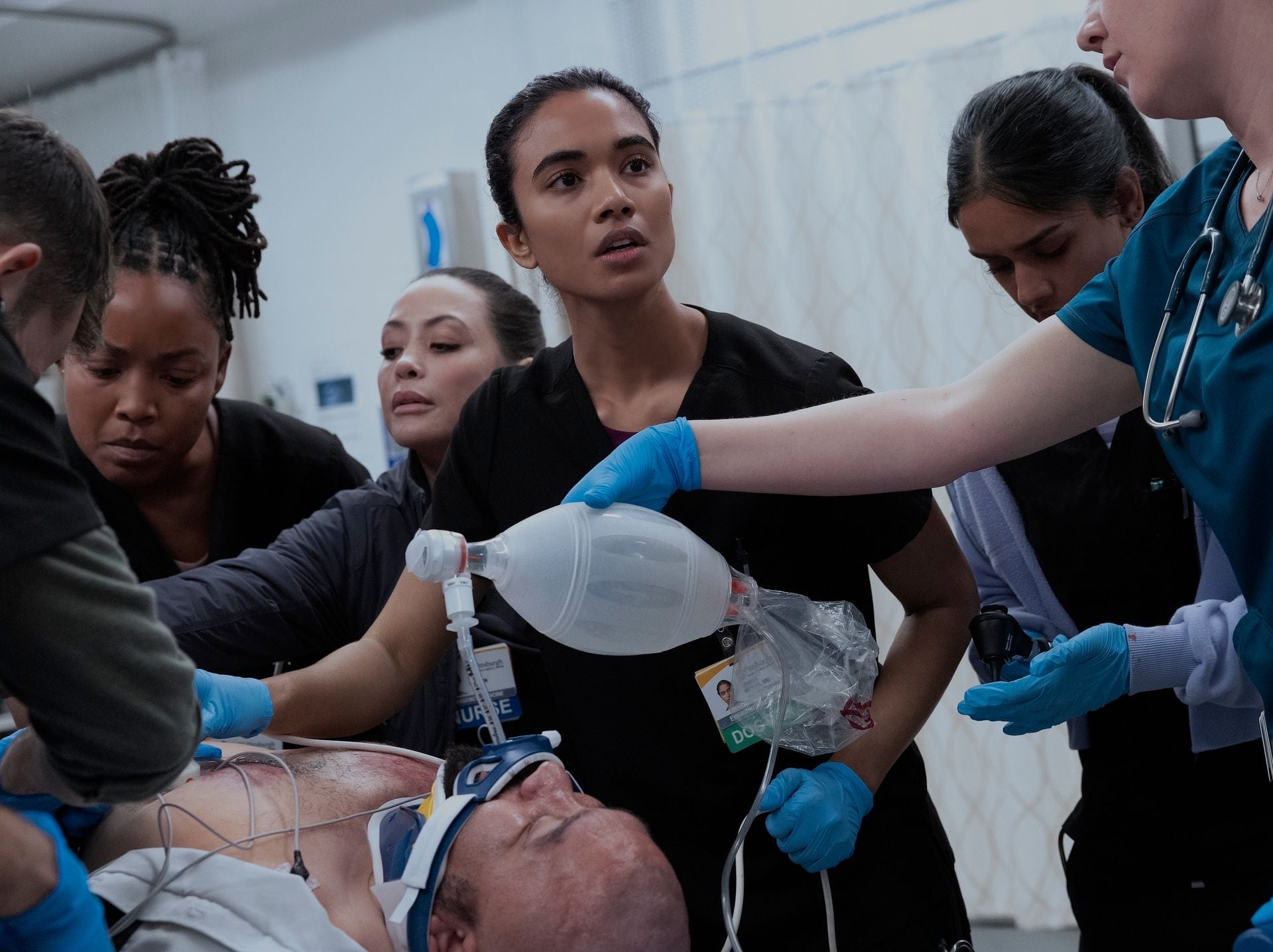
Lit by the cold fluorescence of 21st-century institutional medicine, human illness and raw suffering, medical drama The Pitt, which premiered last year, sweeps viewers into the relentless rhythm of an urban emergency room. The television series, set in the fictional Pittsburgh Trauma Medical Center, has garnered most of the major awards and nominations to which prestige television can aspire, including a raft of Emmys and Golden Globes—with more likely to come.
Both the emergency room and the rust belt city in which it is located conjure hell. In 1868, writer James Parton described Pittsburgh as “hell with the lid taken off”, referencing the flaming cauldrons of its many steel mills. It is here, a century plus later, that the work of treating America’s medical and social ills is allegorised in the show’s unflinching confrontation with physical accidents, diseases and acts of God. Reader beware: plot spoilers abound.


Season one opens with Michael “Dr Robby” Robinavitch (played by Noah Wyle) wading through an overcrowded waiting room into the emergency room (ER). From that point on, the camera never leaves the inside of the ER and viewers embark on a breathtaking, relentlessly mobile journey into the lives and characters found in that space. Immersed in the fascia of an over-capacity ER, we witness, at eye-level, complex, dangerous medical procedures while eavesdropping on fast-paced dialogue worthy of Golden Era Hollywood’s most fluent screwball screenplays.
Through the ambulance bay, EMTs wheel in a never-ending parade of patients in various states of distress and dismemberment. The creator and writer of the series, R Scott Gemmill (who was also executive producer of ER, another hospital drama which ran through the 1990s and 2000s and also starred Wyle), handles medical exegesis and character arcs simultaneously to create a story around patients as self-contained dramatic case studies. Within the show’s “real time” format, each episode encapsulates just one hour in the ER—the 15 episodes of one season match one 15-hour day of endless crises.
The urgency of every emergency is tempered by elaborate gurney choreography and a script and storyline marked by professional hot-dogging and personal anguish. With a dash of flirtation mixed with hazing, seasoned doctors flaunt their skill before their awestruck students, and residents test interns and medical students with procedural and biological banter while performing terrifying intubations and stomach-churning wound examinations.


It quickly becomes very apparent, however, that the doctors and nurses themselves are not well. Dr McKay wears a court-ordered ankle monitor after a physical altercation with her ex-husband’s new girlfriend. Dr Langdon is a pill addict. Dr Collins is (rightfully, as it turns out) worried about her pregnancy. Dr Santos is haunted by what we soon understand is a history of childhood abuse. Dr Whitaker is homeless and squats in a disused wing of the hospital.
Most dramatically, Dr Abbot, a former military medic (played by a grizzled Shawn Hatosy), stands at the very edge of the hospital roof’s ledge at the end of the night shift, apparently contemplating his next move. In the pilot, Dr Robby talks the tough-guy doctor off the ledge, but the theme of suicidal tendencies returns full force in season two. The plot centres on Dr Robby working his last shift before embarking on a three-month sabbatical that he is determined to spend helmetless on a motorcycle. Surrounded by so much death, Dr Robby seems to want to spend his free time courting the grim reaper on his own terms.
“The characters perform their own tortured emotional arcs against a backdrop of an understaffed and under-resourced workplace stretched to its very limits”
Dana, the ER’s charge nurse (played by Katherine LaNasa, with a working-class Pittsburgh accent the internet loves to riff on), is the moral and emotional anchor of the ER throughout both seasons. She tries to talk Dr Robby into getting therapy to mitigate his desire for self-destruction, with Dr. Robby displaying all the avoidant behaviour of a truly traumatised person. Dr Robby’s traumatic material is the centre of the entire series: his professional and managerial expertise are achieved at enormous personal cost.


The characters perform their own tortured emotional arcs against a backdrop of an understaffed and under-resourced workplace stretched to its very limits. In the series one opening episode, Dr Robby has come to work on the fourth anniversary of the Covid-19-related death of Dr Adamson, his beloved mentor in the very ER he now manages. In the thick of the fray of life-and-death emergencies, he is visited by Gloria Underwood, an African American hospital manager dressed in a resplendent pink suit jacket. Gloria’s outfit stands out in contrast to the drab, blood-and-faeces-smeared scrubs worn by the doctors and nurses alike, but her demeanour is grimmer than theirs. She is unhappy about the ER’s low customer satisfaction ratings. She warns Dr. Robby about metrics. We have heard the two nurses, Princess and Perlah, gossiping in Tagalog about a possible sale of the hospital. In the contemporary American moment, the end game would most likely be to a private equity fund ready to strip the Pitt for parts in order to extract short-term profits and a resale.
Gloria is the managerial antagonist American workers know so well. Her focus on efficiency and metrics would make sense in light of a potential sale: in order to satisfy the board, upper management would want to juice the efficiency and satisfaction numbers to get the highest market valuation. Her well-groomed appearance becomes all the more jarring as the shift drags on and the doctors and nurses look increasingly damaged and bedraggled.
Gloria’s poise and confidence stand in stark contrast to the self-doubt and sense of futility experienced by her front-line employees. Dana gets a black eye after being sucker-punched by an unhappy patient and customer. While this might seem like a dramatic device, the statistics on healthcare workers and assault (according to a 2025 study, up to 76 percent of healthcare workers in the US have reported experiencing violence) prove that The Pitt is most emphatically not making stuff like this up.


Season one ends with the ER picking up the pieces after a mass shooting at a local music festival. Dr Robby has a mental breakdown in the paediatric ward where, in a flashback, we see Dr Adamson perish in a Covid-19-era oxygen tank. Caught stealing pills from the pharmacy, hotshot Dr Langdon is dismissed. Dr McKay may or may not be arrested after she was caught tampering with her ankle monitor. And despite her mid-shift miscarriage, critical understaffing demands that Dr Collins returns to work on the ER floor.
“Emotional healing provided by inspired professional leadership shows viewers a way out of social and economic catastrophe”
Dr Robby eventually rebounds and rises to the occasion to inspire his team to fight another day for the people of Pittsburgh. Violence and tragedy are met with competent care and treatment, and the courage and dedication of these heroic professionals washes away the threat presented by Gloria and the administrators regarding the potential sale of the hospital. Season one skilfully and authentically presents emotional healing provided by inspired professional leadership and shows viewers a way out of social and economic catastrophe. Tragedy and triage can co-exist, because Dr Robby is in charge.
However, season two begins with Dr Robby even more burned out and nihilistic than he was when we left him. Private disappointments, including being childless in middle age, haunt him more intensely as he has gotten older. The day is 4 July. We are strapped in for trauma, tragedy and transcendence, but season two of The Pitt seems more formulaic rather than operatic.

The Pitt has a penchant for raising awareness about contemporary public health problems, and many season two episodes feel like public service announcements. The viewer is made aware of and “educated” about social problems and policies. There are the protocols of harm reduction in unhoused people with serious medical conditions; the underdiagnoses of eating disorders among African American women; the determined and masked brutality of ICE agents who are ready to arrest a woman the moment she is treated for a wound. We learn about hacker attacks and ransom demands on hospital databases (this kind of security breach happened in real life at a University of California, San Francisco medical-research institution, where a million dollars was paid in 2020 to get the hospital computers back online). There is the emotionality of palliative care, and undertreated drug interactions in older patients. We see the effects of insulin-rationing on underinsured patients and, finally, the sad fact that emergency rooms are the new church doorsteps: places where infants are abandoned by parents who have no other recourse—be it emotional, financial or medical.
“His embrace of a tiny, vulnerable being is the medicine he needed all along”
In the first episode of this season, an abandoned baby is found in the restroom of the ER’s broiling waiting room. The nurses bring her into the paediatric ward where she is fed and swaddled and named Baby Jane Doe. This baby is impossibly quiet and undemanding, with the reality of the first few weeks of intensive infant care quietly dismissed by the writers. I kept worrying about her, tightly swaddled and all alone in “pedes” (the paediatric section of the ER) under a cold, bright light. As the audience waits for Child Protective Services to whisk her away (they never do), Baby Jane Doe does not add to the chaos of the ER as a real baby would, demanding milk, cuddles, burping, human touch and consistent diaper changes. In this sense, Baby Jane Doe is a prop for Dr Robby’s emotional redemption. She is also Dr Collins’ child lost to miscarriage redeemed.


Dr Robby’s final day at work before his endlessly deferred motorcycle trip culminates with him holding, cooing at, and cuddling the infant. While unsuccessfully trying to convince someone to take Baby Jane home from the ER, Dana delivers exposition on the policy of kinship adoption, a provision that allows healthcare professionals to act as emergency foster parents to children and infants abandoned to their care. With Dr Robby holding the tiny person in his arms, the healer heals himself by putting that warm little body next to his; the doctor’s disappointment with his own personal life, and his sense of futility at a job that overwhelms him and his coworkers, are finally redeemed in this newly formed father/daughter pairing.
Like the ending of season one, season two’s emotional catharsis encourages us to identify with Dr Robby’s humanity in the face of all our troubles. His embrace of a tiny, vulnerable being is the medicine he needed all along. And the infant “Jane” just might be able to put her abandonment issues behind her as she grows and enters her new life as a doctor’s daughter. Social ills find personal solutions. I wanted to criticise The Pitt for all its subtle propagandistic functions, but my eyes filled with tears of relief and happiness for a fictional and temporary happy ending for Dr Robby. I welcomed its sweet, anaesthetising effects as an opioid dream that allowed me to forget, for a minute, the fact that our sad, broken society is increasingly unable to provide for its weakest and neediest members. —[O]
Main image: Taylor Dearden, Patrick Ball and Noah Wyle in _The Pitt _(2025–2026). Courtesy HBO Max/Warner Bros.







A respected voice in contemporary art discourse.
Focusing on ambitious storytelling and insightful art-world commentary. Ocula Magazine publishes in-depth interviews, critical essays and timely analysis on the artists, exhibitions and ideas driving the global art world.
Learn more about Ocula Magazine
Showcasing the best of the art world.
Ocula partners with galleries from around the world to highlight their artists, artworks and exhibitions. Gallery membership is by application and invitation, with each member vetted by an independent panel.
Learn more about Ocula Membership
Specialises in the sale of major artworks.
Led by a team with deep ties to the world’s leading auction houses, galleries and collectors. Ocula’s advisory team offers bespoke services to high-net-worth clients from around the world who are looking to acquire the best of contemporary and modern art.
Learn more about our team and services